

Relapse is the most common cause of mortality in patients undergoing allogeneic stem cell transplantation (ASCT) for acute myeloid leukemia (AML). The presence of measurable residual disease (MRD) at the time of transplant is associated with very high relapse rates, and novel strategies to address relapse risk are needed for these patients. Venetoclax has demonstrated single agent activity in AML, and venetoclax combined with azacitidine, decitabine, or low dose cytarabine is FDA approved to treat newly diagnosed patients >75yrs or older and those unfit for induction. Given the ability of venetoclax to target leukemic stem cells combined with its favorable toxicity profile and ease of administration, we have initiated off label post-transplant venetoclax maintenance for AML patients with MRD at the time of transplant. We report outcomes of our experience to date.
Venetoclax therapy is planned to be initiated approximately 40-80 days post-ASCT upon count recovery (ANC>1000 109/L and platelets>100 109/L) and recovery from early ASCT toxicity. Dose is initiated at 100 mg daily for one week and titrated up by 100 mg weekly to a final maintenance dose of 400 mg daily. Therapy is planned until one year post-ASCT.
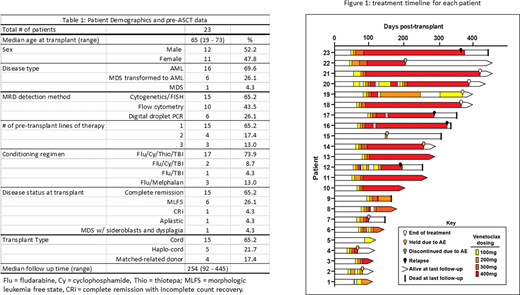
Since February 2019, we have administered venetoclax to 23 post-ASCT patients (22 AML (6 with prior diagnosis of MDS) and 1 MDS), median age 65 (range 19-73). Venetoclax therapy was initiated beginning median 67 days (range 36-146) after ASCT. 16 patients underwent transplant following one line of therapy (twelve of whom received venetoclax azacitadine), 5 patients received 2 lines of therapy, and 2 patients received 3 lines of therapy. Three patients were second transplants. Donor sources were cord (n=14), haplo cord (n=5), and matched related donor (n=4). 7 patients underwent myeloablative, 14 reduced-intensity, and 2 non-myeloablative conditioning. All patients had MRD at time of transplant (15 by cytogenetics/FISH, 10 by flow cytometry, and 6 by digital droplet PCR). At time of transplant, 1 patient was aplastic, 6 were in morphologic leukemia free state (MLFS), one was in complete remission with incomplete count recovery (CRi), 15 were in complete remission (CR), and 1 had MDS with ringed sideroblasts with multilineage dysplasia. Patient data is summarized in Table 1.
Median follow up among survivors is 219 days (range 92-439). Details of individual patients' courses on venetoclax are summarized in Figure 1. In total, 11 patients were still on venetoclax at the time of this analysis, and 4 had completed the planned 1 year of treatment. 3/23 (11%) had the drug permanently discontinued due to potential adverse effects in the setting of additional post-ASCT complications. Four patients relapsed 191, 288, 325, and 367 days post-transplant and all died, and 3 patients experienced transplant related mortality 146, 164, and 307 days post-ASCT. 6 month overall survival (OS) and relapse free survival (RFS) were both 87%. Venetoclax was temporarily held or dose-reduced in 11/23 (47.8%) patients due to adverse events (AEs). 14/23 (61%) patients experienced at least one AE that could be potentially attributed to venetoclax. Most common AEs were cytopenias (7/23, 30%) and diarrhea (7/23, 30%). 12 patients experienced grade 2-4 acute GVHD (3 grade 3). 10 of these patients developed GVHD symptoms prior to starting venetoclax. 5/7 patients who held venetoclax due to diarrhea had acute GVHD prior to initiation of ventoclax, and whether the diarrhea was GVHD or venetoclax related was unclear. Three patients have developed chronic GVHD (2 mild and 1 severe).
Our preliminary data suggests venetoclax is tolerable in the post-ASCT maintenance setting without unexpected side effects. In this small cohort, GVHD rates are comparable to historical controls. Ongoing follow-up will continue to examine the safety and efficacy of this approach.
Pollyea:Novartis: Consultancy; Karyopharm: Consultancy; Takeda: Consultancy; Janssen: Consultancy; Amgen: Consultancy; Pfizer: Consultancy; Agios: Consultancy; 47: Consultancy, Research Funding; Genentech: Consultancy; Glycomimetics: Other; Celgene/BMS: Consultancy; Syndax: Consultancy; Syros: Consultancy; Abbvie: Consultancy, Research Funding; Daiichi Sankyo: Consultancy.
off label venetoclax post-transplant maintenance

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal